
Treatment for erectile dysfunction (ED) is highly effective and safe.
This Medcase offers practical tips for GPs to ensure effective assessment and management of ED.
A reminder: Mechanisms of erection
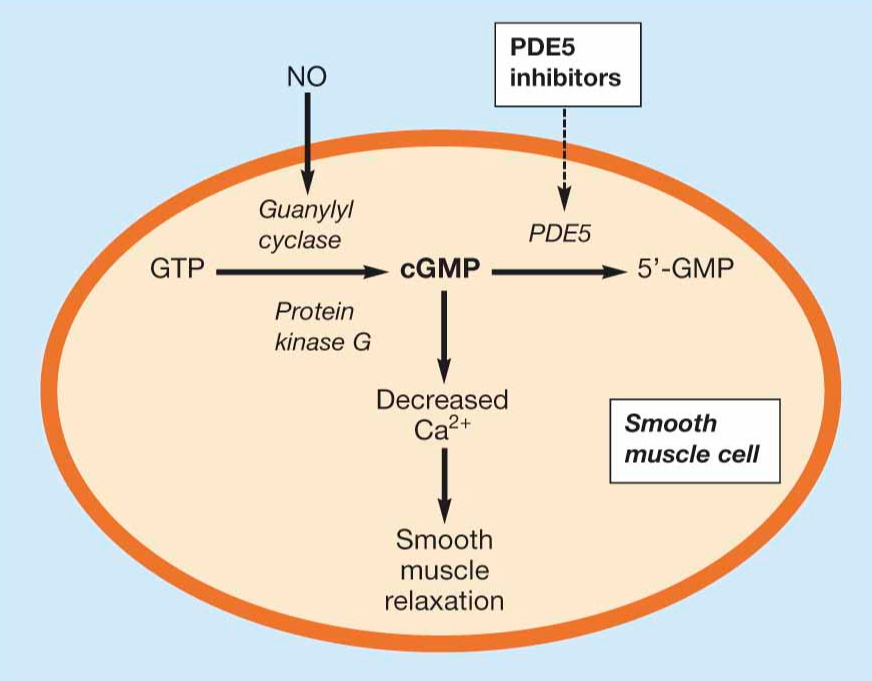
Sexual stimulation triggers the cavernosal nerve to release nitric oxide (NO), stimulating production of cyclic GMP (cGMP) which induces relaxation of smooth muscle of the arteries in the corpora cavernosae.
Blood floods the penile vascular bed and is prevented from exiting by passive compression of the venules.1,2,3 Type 5 cGMP phosphodiesterase (PDE5) degrades cGMP, triggering return to the flaccid state.
Figure 1: Summary of pathways involved in erection (from The impact of erectile dysfunction and its treatment with phosphodiesterase type‐5 (PDE5) inhibitors in patients with diabetes3).
PDE5 inhibitors
PDE5 inhibitors, such as sildenafil and tadalafil, prolong cGMP activity, maintaining erection.1,2,3 They are effective first-line treatments for ED.
In New Zealand, two PDE5 inhibitors are available for prescription: sildenafil and tadalafil. The profile and duration of action vary according to pharmacokinetics, as shown below.
Pharmacokinetics of sildenafil and tadalafil. (from NZ Formulary.)
| PDE5 inhibitor | Time to peak concentration | Mean half-life | Est duration of action |
| Sildenafil4 | 1 hour | 3 - 5 hours | 4 - 8 hours |
| Tadalafil5 | 2 hours | 17.5 hours | Up to 36 hours |
Side effects of PDE5 inhibitors relate to their vasodilatory activity; headache, flushing, hypotension, gastroesophageal reflux and rhinorrhea are possible in response to smooth muscle relaxation.
Sometimes, men experience back, or muscle pain and it is difficult to understand the mechanism of this. PDE5 inhibitors are contraindicated in patients taking nitrates due to the risk of severe hypotension.1,4,5
Food impairs absorption, and a high-fat meal may delay onset of action by up to 60 minutes.
PDE5 inhibitors and cardiovascular disease
ED and cardiovascular disease (CVD) are interrelated; ED is a risk marker for CVD, while CVD can lead to the development of ED.
Vasculogenic ED is the most common type of ED, arising from the same endothelial pathophysiology as cardiovascular disease (CVD) and sharing the same risk factors: age, abdominal obesity, smoking and metabolic syndrome.1
ED symptoms can precede clinically evident CVD by up to 5 years, making it a valuable marker of subclinical CVD.1 Small studies have shown that PDE5 inhibitor-mediated vasodilation can reduce ventricular afterload, leading to improved cardiopulmonary function.
They may also act directly to improve endothelial function, improve insulin sensitivity and enhance microvascular blood flow.1,6,7,8
Observational and retrospective analyses show that PDE5 inhibitors are associated with improved CVD outcomes in men with existing coronary artery disease or a history of previous MACE (major adverse cardiovascular events). PDE5 inhibitors were associated with dose-dependent benefits, including:
- reduced overall mortality
- reduced incidence of MACE
- fewer hospitalisations for heart failure.1,6,7
So, should everyone with ED take a PDE5 inhibitor for CVD prevention?
No.
Prospective, randomised controlled trials demonstrating a causal link between PDE5 inhibitors and cardioprotection are currently lacking. Data thus far are limited to basic science, which describes mechanisms by which PDE5 inhibitors can improve cardiometabolic health, and retrospective or observational studies showing an association between PDE5 inhibitor use and improved cardiovascular outcomes.1 It’s too soon to be certain of clinical benefit.
For now, GPs should focus on understanding who is most likely to benefit from PDE5 inhibitor therapy and how to optimise the use of these medications, given that there may be a cardioprotective association.
Before prescribing: Risk stratification
Men with ED should be considered at risk for potentially sudden fatal cardiac events until proven otherwise.1
Presentation of ED is an opportunity to review cardiovascular risk.
Occasionally, a man presenting with ED may have significant cardiovascular or peripheral vascular disease, which needs treating in its own right. If a man might potentially need a nitrate medication or if his exertional capacity is less than walking two flights of stairs (the accepted medical exertional capacity ‘requirement’ for intercourse), then treatment may need to be deferred until the cardiovascular situation is investigated and treated.
More commonly, ED may be a marker of endothelial dysfunction and co-exist with metabolic dysfunction.
It is an excellent opportunity to screen for these, and men will often be quite motivated to address these issues when they can see links between their lifestyle, medical metabolic risk factors and erectile function.
Risk Stratification of Patients with ED Based on the Princeton IV Guidelines1
| Risk Category | Recommendation |
| Low • Sexual activity does not represent significant cardiac risk (they can climb 2 flights of stairs without cardiovascular symptoms) |
These patients can be safely treated in primary care with no need for further testing. |
| Intermediate or Indeterminate • Mild-moderate angina pectoris • Previous MI without intervention awaiting further stress testing • Congestive heart failure (NYHA functional class II) • Non-cardiac sequelae of atherosclerotic disease (peripheral arterial disease, stroke, TIA) |
These patients require further stress testing before resuming sexual activity, such as completing 4 minutes of the standard Bruce Protocol Treadmill Test (5-6 METS) without symptoms, arrhythmias, or a fall in systolic BP. |
| High • Severe or unstable cardiac conditions that pose a significant risk with sexual activity |
These patients should defer sexual activity until their condition is stable. |
A useful question to determine whether sexual activity is likely to precipitate angina is:
“Can you climb 2 flights of stairs without feeling chest pain or shortness of breath?”
Sexual activity is estimated to correspond to a workload of approximately 2 to 3 metabolic equivalents of task (METS), equivalent to climbing 2 flights of stairs.1 Patients able to climb 2 flights of stairs are likely to be low risk and use of PDE5 inhibitors is safe.
Examination and investigations for other causes of ED may be required; a full discussion of work-up for ED is beyond the scope of this MedCase but can be found in this bpacnz article: Erectile Dysfunction.
How to optimise the use of PDE5 inhibitors
When initiating a PDE5 inhibitor, ensuring a shared understanding of safe, effective use is important.
Patients should be reassured that most adverse effects are unpleasant but not dangerous.
Some young men with minimal physiological dysfunction may find sufficient benefit from occasional use. However, most men will require an intentional programme of use to experience benefit.
Successful use of PDE5 inhibitors is much more likely after counselling about partner expectations and education about trialling the drug at least 8 times, titrating to maximum dose, and using it regularly.1
Practice Tips
Tips from Dr Alistair Somerville (MBCHB FRNZCGP DipClinEd).
- Start high: initiate treatment with a full dose to enhance certainty of effect.
- Use without a partner initially to remove psychological barriers.
- Encourage regular use (2 to 3 times per week) to build confidence.
- Trial a minimum of 8 attempts before assessing efficacy.
- Food, especially a high-fat meal, impairs absorption and may reduce effectiveness; advise to take 30 minutes prior to a meal.
- Alcohol potentiates vasodilation; it can reduce effectiveness and increase vasodilatory adverse effects.
After prostate cancer: Recognise and treat early
85% of men will have erectile dysfunction following prostatectomy.9 Rate of recovery is low (16% in men <60 years, 6% in men >60 years) and may take 18-24 months, if it occurs. In the interim, men may experience penile atrophy.
It is important that men are prescribed a trial of regular PDE5 inhibitor medication, to commence as soon as they feel ready following their operation. This ensures vasodilation of the penile arteries and ongoing blood and oxygen supply to the penile tissues.
However, because the mechanism of the erectile dysfunction is injury to the cavernosal nerve, rather than endothelial dysfunction, PDE5 inhibitor treatment is only successful in about 15% of men with ED following prostatectomy.
If there is no response to a 2-3 month trial of regular PDE5 inhibitor treatment, consider referring the man to a medically robust, caring provider for consideration of intracavernosal injection treatment. When done carefully, this is well tolerated, safe and effective. PDE5 inhibitors are safe and effective in this setting and should be recommended as a first-line treatment. Advise regular use, 2 to 3 times weekly for a minimum of 1 month.
If there is an insufficient response, other therapies, such as intra-cavernosal injection, may be indicated, and further advice should be sought.
This MedCase was written by Dr Vicki Mount, BSC/BCom, MBChB, MRNZCGP, DipPaeds, with expert review by Dr Alistair Somerville (MBCHB FRNZCGP DipClinEd).
References
Recognition of Learning Activities
Don't forget to log your time with The Royal New Zealand College of General Practitioners portal for recognition of learning activities.

